回复: 关于两个寿命帖子的思考
谢谢上面所有各位。
观察角度的探讨不错,
技术角度的探讨更好。
麻烦适应这里生活的,英文好的同学,帮忙分析一下,翻译方面的问题:
http://www.statcan.gc.ca/pub/82-622-x/2011008/findings-resultats-eng.htm
China, India and the United Kingdom
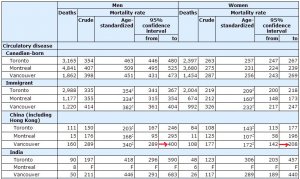
China (including Hong Kong) and India have been leading source countries since the 1980s; the United Kingdom had been a major source country in earlier years. A healthy immigrant effect was apparent among immigrants from each of these birthplaces (data not shown). Among men, at the national level, ASMRs were 690 for those from India, 810 for those from China, and 1,105 for those from the United Kingdom; this compared with 1,305 among Canadian-born men. Among women, the ASMRs were 537 (India), 471 (China), 695 (United Kingdom) and 731 (Canadian-born).
At the CMA level, ASMRs for immigrants from each of the three countries were generally lower than those for the Canadian-born (
Table 3). The exceptions were women from India living in Toronto (634) and Montreal (503) and women from the United Kingdom in Vancouver (700), whose ASMRs did not differ significantly from those of Canadian-born women.
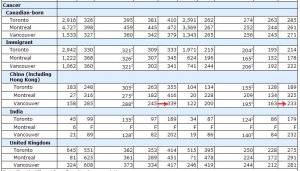
The elevated ASMR among women from India at the CMA level largely reflected a high circulatory disease ASMR (Appendix
Table H). In Vancouver, the relatively high ASMR among women from the United Kingdom was partially due to high ASMRs for circulatory disease (289) and for cancer (281). Immigrants from China almost always had lower ASMRs, compared with those of the Canadian-born population in each CMA. However, in Montreal, the cancer ASMR among women from China (209) was similar to that of Canadian-born women (252).




 Very constructive and positive points!
Very constructive and positive points!
 遭遇砖头阵。
遭遇砖头阵。